Mr. Jones is a 58 year old gentleman who was referred to Melbourne Urology Centre with bothersome urinary symptoms. Mr. Jones had been experiencing these symptoms for quite some time, however they were becoming increasingly frustrating to deal with and impacting his quality of life. With some encouragement from his wife, he made an appointment with his GP, who ran some preliminary tests before referring him to consult with a urologist.
Mr. Jones was diagnosed with benign prostatic hyperplasia (BPH), and following consultation with the urological surgeon, opted for Rezum treatment.
Symptoms and initial GP assessment
The symptoms that Mr. Jones presented with were very common to male patients with benign prostatic hyperplasia (BPH), also sometimes referred to as prostate enlargement. These urinary symptoms included:
- Straining and difficulty to begin urination
- Weak urine stream
- Stop/start flow of urine
- Urgency to urinate
- Frequent urge to urinate overnight (nocturia), causing disturbance to his and his wife’s sleep.
Mr. Jones’ GP performed initial tests which included a urine test, PSA blood test and ultrasound. The urine sample was normal, with no blood or signs of infection. PSA (prostate-specific antigen) test was 1.2- normal for a man of his age. The ultrasound showed an enlarged prostate, measuring 60cc (normal size ~30cc) with incomplete bladder emptying.
The GP suggested a trial of medication. Tamulosin was prescribed, however this caused undesirable sexual dysfunction for this patient. Mr. Jones was then referred to Melbourne Urology Centre.
Consultation with a urologist
During the consultation with the urologist, a thorough assessment of Mr. Jones’ condition was performed. This included examination of the patient’s medical and family history. Mr. Jones did not have a history of prostate cancer in his family, however his father did have an enlarged prostate. The urologist assessed the prostate, and no sign of cancer was detected.
A flow test was performed at the urologist’s rooms, which showed slow flow and incomplete emptying of the bladder.
Rezum treatment for BPH
All of the treatment options were discussed with Mr. Jones. The patient noted that he preferred not to take medication.
Mr. Jones opted for Rezum therapy for prostate enlargement, due to the fast recovery time, less bleeding and less risk of sexual dysfunction than traditional surgery. He had an uncomplicated procedure, stayed overnight in hospital and was discharged the following morning.
Outcomes of Rezum treatment for prostate enlargement
Mr. Jones noted an improvement in his urinary symptoms after a few weeks, with better urine flow and bladder emptying. As expected, the bladder symptoms of frequency and urgency to urinate improved after a few months with bladder retraining, as guided by the urologist.
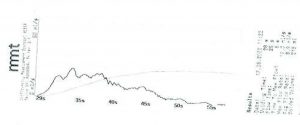
Flow rate results following Rezum therapy indicating a maximum flow of 19 mL/sec.
If you would like to discuss Rezum treatment for prostate enlargement or other treatments for BPH, please speak to your GP and obtain a referral for one of our urologists at Melbourne Urology Centre.
This case study is unique to the individual patient as described and the name has been changed to ensure patient confidentiality. Treatment details should not be taken as general medical advice. If you are suffering with BPH or urinary symptoms, please consult your GP or urologist for a thorough assessment and personalised treatment plan.